Shawna Mastro Campbell, Bond University; Melanie J. Zimmer-Gembeck, Griffith University, and Tanya Hawes, Griffith University
Children thrive when parents are warm and responsive to their needs, while also providing clear guidance and setting limits. This is known as authoritative parenting.
But most parents will tell you authoritative parenting is easier said than done, especially when children have frequent intense emotions, big behaviours, meltdowns and outright defiance.
These challenges can lead parents to wish they had a parenting coach helping them know what to do and say.
Parent-child interaction therapy aims to do just that. It has been used in parts of Australia for around 20 years and is now available in some western Sydney schools.
So how does it actually work?
It focuses on the relationship
Parent-child interaction therapy is based on attachment theory, which posits that quality relationships in childhood predict wellbeing.
The parent and child play together in one room while the therapist observes in an adjacent room through a one-way mirror.
Using an ear-piece and microphone (or other communication device), the therapist acts as a coach to guide a parent’s responses to their child during play.
Coaching guides parents as they use positive attention skills to respond to their children’s behaviours and emotions as they occur. Within such a supportive environment, this reduces the child’s problematic behaviour and increases appropriate behaviours.
This guided, real-life practice gives parents the ability to use the techniques on their own, wherever they are, and enriches the parent-child connection.
How do kids experience it?
Parent-child interaction therapy was was first used in the 1970s to treat problem behaviours of children aged three to seven years. It’s now used from 15 months of age.
Although the child can’t see the therapist through the mirror window, they are aware their parent can hear the therapist through the earpiece.
From the child’s perspective, the play environment is often enjoyable and they get to spend high quality one-on-one time with their parent, enhancing the relationship.
Parents learn the importance of their attention
Throughout the therapy, the parent directly experiences the importance of their own attention.
When children get their parent’s attention for disruptive or other challenging behaviour, such as yelling, this can escalate children’s disruptive behaviour over time because parental attention makes any behaviour more likely to occur.
Children will even seek this attention if it comes in the form of a parent yelling, correcting, or negotiating, especially if they get little connection or attention when behaving appropriately.
In parent-child interaction therapy, parents use attention to reinforce their child’s positive behaviour. They practise giving positive attention for appropriate behaviour, such as praising and showing enthusiasm for children’s patience, kindness, good listening, or sharing.
The therapy also encourages parents to limit attention to unwanted behaviour when it’s safe to do so. A parent may be coached to avoid acknowledging when a child uses inappropriate language or “toilet talk”, for example.
Practising these attention strategies can increase children’s positive behaviours and interrupt the cycle of worsening behaviour and negativity.
Parents practise authoritative parenting
During parent-child interaction therapy, parents practise real-time strategies for authoritative parenting that:
- demonstrate warmth and responsiveness to their child’s needs
- fairly and clearly state expectations for behaviour
- are consistent in developmentally appropriate consequences, especially for aggressive behaviour.
Coaching focuses on responding kindly, while still setting clear boundaries and expectations for behaviour.
For example, by saying:
Thank you for following the rule of being gentle today. I really like when you do that at home with your brother, too.
Who is – and isn’t – it suitable for?
Research from Australia and abroad shows this type of therapy can be effective for behavioural and related emotion regulation problems.
It has also been shown to be effective among culturally diverse families and those who have faced adversity or have complex health and mental health challenges.
Research shows additional benefits for parents. These include reduced stress, improved parenting skills and confidence and improvements in the ability to manage difficult emotions such as anger.
Parent-child interaction therapy is most often used for children with conduct disorder, oppositional defiance disorder, and trauma-related conditions, as well as conditions where behaviour concerns can be a symptom, such as attention-deficit hyperactivity disorder (ADHD) and autism spectrum disorder.
However, it can be used for children without any mental health diagnosis
It’s not recommended when there are safety issues or unstable relationships in the family or home environment. In these instances, other interventions should be prioritised over treating children’s behaviour concerns.
The downsides
Parent-child interaction therapy is time consuming and resource intensive. Therapy typically lasts 14 to 16 weeks, with most sessions involving both parents and children. Research shows repeated practice can lead to more sustained improvements in children’s behaviour. So it can involve a big commitment from parents.
Parent-child interaction therapy is delivered by qualified mental health service providers such as registered psychologists and social workers. They require extensive training, ongoing professional development and program training from an approved provider, as well has months of supervised practice. They also require specialised rooms and equipment. This can limit access.
Currently in Australia, the program is offered at a few universities and in some school settings, with costs often offset by public funding. There are few private providers.
Behaviour problems are the most common reason parents seek support for children. Supporting them with evidence-based programs or therapies – whether that’s parent-child interaction therapy or others – can deliver wide-reaching benefits across their lifespan.![]()
Shawna Mastro Campbell, Associate Professor in Clinical Psychology, Bond University; Melanie J. Zimmer-Gembeck, Professor of Psychology, Griffith University, and Tanya Hawes, Program Co-ordinator/ Psychologist, Griffith University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
 Rancho Cordova police deputies deliver baby (Released)
Rancho Cordova police deputies deliver baby (Released) Krista Richard with Younis and Aws, two children who received one of her free bikes – credit, supplied by Richard to GNN
Krista Richard with Younis and Aws, two children who received one of her free bikes – credit, supplied by Richard to GNN


 Kim Smith – SWNS
Kim Smith – SWNS (Photo: AI generated image/IANS)
(Photo: AI generated image/IANS) – credit Leighann Blackwood
– credit Leighann Blackwood
 Powerlifter Martine Barons competing in Squat at the European Championships – SWNS
Powerlifter Martine Barons competing in Squat at the European Championships – SWNS Powerlifter Martine Barons on winners platform at European Championships – SWNS
Powerlifter Martine Barons on winners platform at European Championships – SWNS SWNS
SWNS credit – Maggie Boynton, retrieved from TikTok
credit – Maggie Boynton, retrieved from TikTok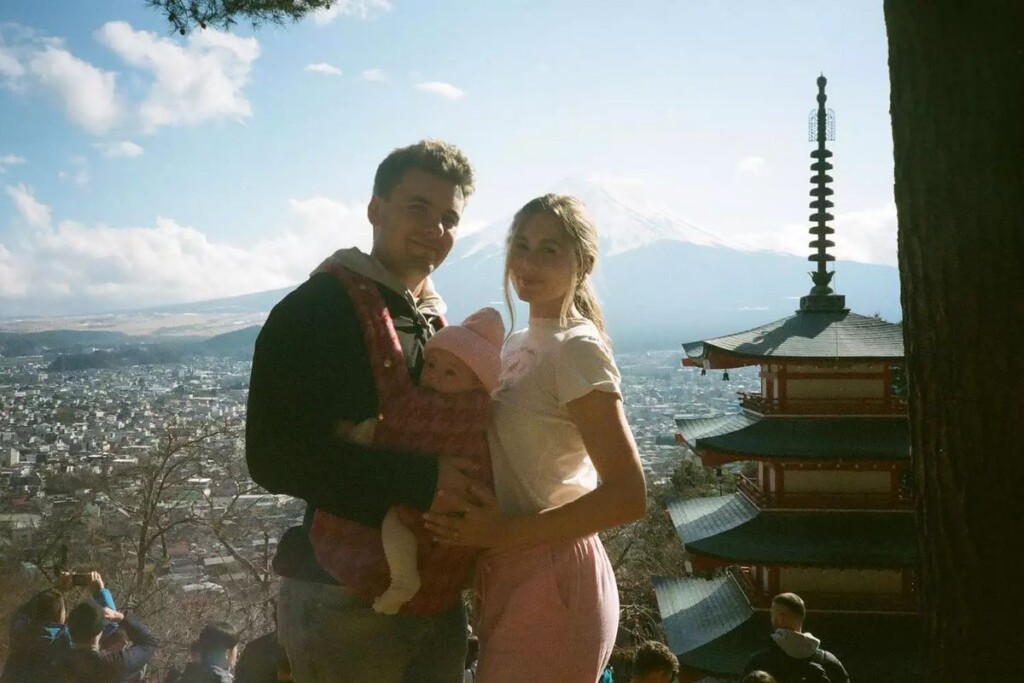 Maggie Boynton and her husband with their daughter in front of Mount Fuji – credit Maggie Boynton, retrieved from TikTok
Maggie Boynton and her husband with their daughter in front of Mount Fuji – credit Maggie Boynton, retrieved from TikTok Lost and found rings – Courtesy of Laura Emanuel and Jeffrey Laag
Lost and found rings – Courtesy of Laura Emanuel and Jeffrey Laag


 Magda Berg with her two sisters Beata and Daria -via SWNS
Magda Berg with her two sisters Beata and Daria -via SWNS Magda Berg as a child – via SWNS
Magda Berg as a child – via SWNS Magda Berg with her sister – via SWNS
Magda Berg with her sister – via SWNS





.jpg){kind=link}